 |
|
|||||||||
|
|
|
|
|
|
|
|
||||
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|

Heart Health
The Heart Solution
Note: this is a transcription from a talk given by Dr Richards.[Contact the RFHC for a copy of this audio tape, The Heart Solution]
I've been putting more and more attention to cardiovascular disease and heart conditions recently. The simple reason for that is the more I learn, the more startled I am by how completely out of sync with our expectations our current medical care for heart trouble actually is. This is the latest information about the common medical protocols including medication and the surgeries that are currently used. This information is really startling. And I want to talk more about some of the successes we've been having at the Center a phonocardiogram or an acoustocardiograph, We have a common sense approach to heart trouble. It is not a mystery, in spite of what we may have been led to believe.
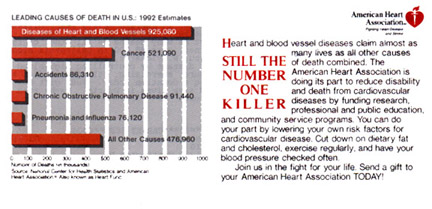
Every year the American Heart Association puts out a little chart, they send it out with their request for annual donations, and it's always the same, it varies by a few hundred thousand people here or there, sometimes a few ten's of thousands, but the number one killer in the United States is cardiovascular disease, that is disease of the heart and peripheral vessels. That's heart attacks, strokes, coronary artery disease, all of those things are lumped in under that heading. By far the majority of it is disease of the arterial disease in one way or another, most heart attacks are a result of coronary artery blockage, most strokes have that common feature to them, there's some kind of pathology that is creating the embolus that eventually causes the stroke. What you may not be aware of is that there's a wealth of information that shows that we are losing the battle against cardiovascular disease in this country. A study published in the New England Journal of Medicine, in fact, they followed this study long-term and they published the results in '86, '87 and '91 showed that people who are taking multiple cardiac medications have 40 percent higher risk of mortality after 4 years than those people who take nothing. Now most us who go to a doctor to take a medication don't think that that's going to be the risk we're facing but that's what's happening. There was a long-term study in Finland that was published in The Journal of the American Medical Association in 1991 that showed the same thing, that there was far higher mortality with multiple medications. There was a European study of 10,000 men, there was no increase in survival with multiple medications and that was in the European heart journal in 1986. The Journal of the American Medical Association reported on a study of 12,000 men with the same results. There was a World Health Organization study, this was published in Lancet and was done all through Europe, 61,000 men, the same result. The medications were either increasing mortality or there's no increase in survival time. And in fact the British arm of the study which was published in Lancet showed an 8 percent increase in mortality. Another interesting comparison is between the United States and Canada. The US is very aggressive compared to Canada. We have 11 times the rate of angioplasty surgery and 10 times the rate of bypass surgeries but the survival times are virtually identical between the two countries. And this was published in the New England Journal of Medicine in 1997. Now do you find any of that information kind of shocking? We're not hearing this from our medical doctors, I don't think. Most of us go and think we're going to be helped. It's very important that you know I'm not making this up out of my head and if anybody wants to look up the references I've got them all.

This little graph recently came out in our chiropractic newspaper and I thought this was just a fascinating chart and I wanted to share it with you. The top graph shows elderly patients without appropriate prescriptions, without conflicts in their prescription or the wrong prescription. Do you notice that the best number up there is 57 percent? Isn't that 57? People who have less than 4 prescriptions, 57 percent have the right thing. That means 43 percent of them are being given inappropriate or dangerous medication. That's scary. And the numbers rise as you look at the more the medications, the larger the numbers of inappropriate medications until you get to where people who are taking 6 or more drugs, or is that 8 or more drugs, and there's only 7 percent of those people who do not have inappropriate medications. I'm not actually surprised by this because I take extensive drug histories when people come in for consultations and I almost always find that one of the drugs someone's taking is for the side effects of another drug or they interact with each other or even worse it's contraindicated for whatever's wrong with this particular person. A lot of people with heart failure are being given beta blockers and they're contraindicated for anyone with heart failure.
I was fascinated by the statement that came out at the first of the year that deaths from cardiac failure are increasing dramatically, while deaths from heart attacks have declined slightly. This was actually published in Lancet in Britain in 1993 and it came to this country to the news press at the beginning of the year. The fact is that there are several classifications of drugs that are widely used in this country for people with heart conditions that cause cardiac failure, so what that statistic means is that we're seeing a rise in iatrogenic or doctor-caused heart failure, that's really what's happenning. The other thing is that the new hot button is homocysteine. Have you heard that? I've had about six or eight people ask me about homocysteine within the last three weeks. It's interesting how things get to the popular press and then I start getting questions on them. And when you hear about this the way it's presented it sounds like there must be some magic drug that will reverse homocysteine levels, well what it actually means is that your body is B-vitamin deficient. If you have high levels of homocysteine in your urine all it means is that you don't have enough folic acid and vitamin B6 to break this toxic thing down to its proper metabolyte, I can't even remember what it is now, so it can be excreted safely. So it accumulates in your arteries and it damages your arteries. All it is is a sign of a nutritional deficiency. And we have a lot of those in our culture including birth defects, we found out. So B vitamin deficiency is incredibly widespread in the United States and this huge rise in cardiovascular disease is one of the symptoms of it.
[TOP]
And there are two major therapeutic models in medicine. The first one is surgery, the second one is medications, either or. That's what they do with these conditions. Bypass surgery is risky business, and I have to apologize, I told you I had all the references. I looked everywhere, I read this first thing within the last two weeks and now I can't find the article that I read it in, but I was just stunned because for some private hospitals bypass surgery is 30 to 40 percent of their income. And the percentage of bypass surgeries are going up so fast it's unbelievable and in fact there are 250,000 of them performed every year in the United States which represents an 8 to 12 billion dollar income for the medical profession depending on how much they charge at any given hospital. The rates vary according to what part of the country you live in. Out here they're very expensive. And the post-operative complications of bypass surgery include brain damage in approximately a third of the patients, they have some form of brain damage which will often include personality change because the frontal lobes are often affected. Five percent of the people die in the surgery on the table. There's more than 1 in 20 of the people who have bypass surgery who suffer a stroke shortly thereafter, that was in the New England Journal of Medicine in 1996. Now this might all be okay, I mean you might think the risk is warranted if the procedure was effective, right? Well by our statistics only 21 percent of the surgeries are considered effective and 50 percent of these arteries clog again within 5 years because very few people who are given a bypass surgery are given any counseling about how to change their lifestyles so it doesn't happen to them again. Um, angioplasty is the other surgery that they use with the little balloon? You know where they go smash, smash. Well there was an article in the New England Journal of Medicine just this year in 1997 that shows that angioplasty isn't as effective as bypass surgery in symptom control because 60 percent of the people who had angioplasty had to have further treatment because their arteries just started clogging up again and they weren't able to perform daily activities as well as those who'd had bypasses like housework and walking the dog and that kind of thing? They just couldn't do it. And 26 percent of them continued to suffer from angina, whereas with bypass surgery the percentage is about 11 percent. And there was an article in New England Journal of Medicine in '96 that showed the outcomes for angioplasty were no better than the drugs and we already know the drugs aren't very good, right? And unfortunately both of these procedures only added 4.4 years of life on average to the lives of the people who underwent them. So that was in the New England Journal of Medicine in '97. So there's a lot of risk involved for what some might consider to be marginal amounts of benefit. And the more important that I really want to stress here is that the coronary arteries are only one set of arteries in your body. You know the best way to diagnose coronary artery disease? Look in somebody's eyes. If you look at the back of their eye at their retina you can tell if they have arterial disease so that says this process is taking place all over your body, right? So going in and taking out the artery surrounding your heart is not solving the problem. It's just trying to give you some palliative relief.
MAJOR CLASSIFICATION OF CARDIAC DRUGS
Vasodilators
Anti-hypertensive
Beta-blockers
Anti-arrhythmics
Anti-platelets
Cholesterol lowering drugs
Now the other major classification of treatment are cardiac medications and basically there's six major types: vasodilators, antihypertensive, beta blockers, antiarrhythmics, antiplatelets, these are the things that prevent platelet coagulation, not all of them are anticoagulants although that's kind of how we think of them, and the cholesterol lowering drugs. And I'm going to go through each classification of these drugs so that if you're on one of them you can kind of get an overview of what you might expect.
[TOP]
The vasodilators are two basic kinds: nitroglycerine, and nitroglycerine analogs as well as calcium channel blockers. The nitroglycerine analogs include things like indur, nitrodur, nitrobid, sorbitrate, hydralazine, and dilatrate. I can't even say a lot of these names. And that's not an exhaustive list, it's a partial list of some of the more common ones, okay? They cause side effects like headaches and dizziness. The problem, the biggest problem with them is this potentially fatal alteration in heart rhythm. The heart can either slow down so far so that you don't get enough of a beat, enough of an effective beat or it can speed up really fast. And they can cause extreme low blood pressure. Now calcium channel blockers although they're also considered to be vasodilators, have a whole different set of side effects that go with them. Calcium channel blockers are things like cartizam, and calen, procardia, I don't know that procardia is used as widely anymore. There was a whole book on procardia that came out some years ago because it caused irreversible fibrosis in people and it was just a horrible - you know, it was lifethreatening. So, but some people are still on it. It causes things like constipation, vomiting and G.I. bleeding, water retention, these sudden, rapid heartbeats, more serious are the liver disorders that these drugs can cause, and the rashes are secondary to a really severe allergy to the medication and depression. There was an article in the Journal of American Medical Association, in fact there were two articles in 1996 warning against the use of Procardia niphedipine because it causes this initial drop in blood pressure and then 5 hours later a really steep rise so it was increasing the incidence of heart attacks and they were warning doctors about that. And then in Lancet in 1996 there were two articles, one warning that calcium channel blockers will double the risk of developing a malignancy, and also because they reduce coagulation time so far they can cause severe gastrointestinal bleeding in the elderly, you can get hemorrhage. Most of what you see up here where it talks about G.I. disturbances, it's gastrointestinal hemorrhage, which is a life threatening condition. Now our antihypertensive drugs which is the next class we're going to consider. Again we have two classifications here, one are the ACE inhibitors, the acetylcholine inhibitors, and the others are the diuretics. We also have potassium channel blockers but they're not as commonly used. Our ACE inhibitors include things like Acupril, Capatin, Lotensin, Monopril, Zestril, Vasotec, maybe some of those names are familiar, right? And our diuretics come in two different varieties, we have potassium wasting and potassium sparing. The potassium sparing diuretics are really the most dangerous because excess potassium is very hard on the heart. It weakens your heart and it weakens the effectiveness of the contraction and boy it can cause heart failure just that fast. Potassium sparing diuretics are things like aldactazide, aldactone, midamor, diazide, maxzide, and our potassium wasting ones are things like hygrton, enduron, diuril, or there's a whole list of them, perhaps the most common and familiar one is Lasix, everybody's heard of Lasix, right? So the ACE inhibitors can cause these sudden drops in blood pressure together with dangerous rise in the potassium levels and the problem that sometimes occurs is that people go on the ACE inhibitor together with the potassium sparing diuretic like aldactazide together with lotensin and that's a really dangerous condition. It could actually cause fluid on the lungs, pulmonary edema, which is a life threatening condition. Some of the other side effects include things like kidney malfunction and muscle cramps, diarrhea, nausea, fatigue, rashes, or abdominal pain, heart palpitations, jaundice, sleep disturbances, mood swings, and impotence. And when we come back to our diuretics we're looking at G.I. disturbances again because we can get ulceration and bleeding from some of these products, dry mouth, skin rashes, photosensitivity, kidney damage and pancreatitis. That's a pretty long list of possible adverse effects and in my experience of working with people on heart medications they're usually being medicated for at least one other condition that they have which is very often a side effect of the drug. I've seen that over and over again. Let's talk a little bit now about beta blockers. I don't want this to be a huge litany but I just want people to be as informed as possible. Beta blockers, Tenormin, Lopressor, Biocardin, Normadine, Korguard, Tinoptic, Indural, there's some new versions of this where they put them together with diuretics, Induride is one of those and Tenortech, that's another one that's a combined form. If there's any class of medication I hate I hate beta blockers. We now use beta blockers for children with asthma, seldane, right? It's a beta blocker. The problem with beta blockers is that they force you into heart failure. There are any number of warnings in the PDR that beta blockers are very dangerous for people who have arrhythmias, for people who have a heart block because it lowers cardiac output so far and makes the heart muscle flabby so before you know it you've got heart failure. I have a very dear friend who died, he had had a massive heart attack, he was on beta blockers for 12 years and he died of heart failure. And the physician's' assistant who was a very nice man said well of course because we all know that that's what beta blockers do. It's like giving you a life extension but it only lasts for 10 to 15 years. They can also exacerbate asthma and in some people they can cause asthma, a lot of fatigue with your cold hands and feet, sleep disturbances, nightmares, again we have stomach upsets because you have beta adrinurgic receptors in every part of your body, the bronchioles, the gastrointestinal system, and the artery. So these things effect your whole system and you can't digest food after a while if you've been on them long enough it's like you can't digest anything because your whole digestive system is shut down and you're not making the right hydrochloric acid to break down your proteins. So stomach upset is really common with these and a lot of rashes. Tinormin was reported in the Journal Hypertension in 1996 to double the risk of kidney cancer in hypertensive patients. And Lancet, again this is a British publication in 1996 reported in a study using beta blockers that they actually stopped because the side effects were so alarming and there was an editorial in that issue of Lancet that stated about this research, we must assume that all anti-arrhythmics are potentially fatal. That's a very strong statement for a respected medical journal and Lancet is one of the most respected journals in the world. So I don't like beta blockers. Then we have our anti-arrhythmic drugs. This is the classification of drugs where they give people who have like ventricular fibrillation and atrial fibrillation, you've heard of digitalis, well Lanoxin and Digoxin and all of these drugs are synthetic forms of digitalis. Digitalis and its derivatives are the most toxic drugs in the world They have the smallest margin of error when you study pharmacology and toxicology there's this concept of lethal dose, what is the dose that will kill half the population to whom you give it? And then what's the dose that's safe. And that margin that you get in between tells you how much room you have to play. Digitalis has the most narrow margin in the world. As well as do the synthetics that are wrought from it. So the side effects of these antiarrhythmics include things like heart failure and chest pain, a lot of people get a choking sensation like they can't swallow, lightheadedness, impaired vision, some people get skin discoloration with it, it's a side effect of the ineffective blood flow, phototoxicity (can't go out in the sun because you get real sensitive to it), diarrhea and fever, the lupus like symptoms which again go with the phototoxicity, and in some cases frank liver damage and psychosis. In The New England Journal of Medicine in 1991 they reported on a study of people taking antiarrhythmics. Eight percent of those people in the study died fronm arrhythmias compared to 2.2 percent who took the placebo. Four times as many people died on the medication than those who were taking the placebo. This was a controlled double blind study, they didn't pick out the good guys to not take it, they were all equally ill. And in that same study 3 percent of the people on the medication died from heart attacks compared to less than 1 percent who were in the placebo group. So there are some serious questions about the efficacy of these drugs as well. Then we have our antiplatelet drugs. You know an aspirin a day? You've heard that, right? This is part of that. There are some stronger ones that they used, they used warfarin and coumadin as well, heparin used to be used but it's not used quite as widely anymore. There are some prescriptions that have aspirin in them like Ecotrin, that's a coated enteric aspirin to protect the stomach. All those things are included in this class. Again we have our GI problems, this severe bleeding. And the respiratory disorders are also about bleeding. The thing about aspirin that is different from the other is that aspirin will cause metabolic acidosis and for people with asthma that's a real serious problem so they can get into respiratory distress really easy. And if you have people that complain of ringing in their ears the first things you need to ask them is are they taking aspirin every day? That's the most common cause of that tinnitus because it changes the p.H. in the bloodstream. Stroke is also a side effect of these drugs because it's real easy to give somebody too much and then they start bleeding into the brain and that's basically what a stroke it. Diarrhea, vomiting, throbbing headaches and very low blood pressure. We have one more classification of drugs we're going to talk about and then we're going to start talking about the good stuff, okay? You know, cholesterol lowering drugs are becoming so common that they're quickly moving up on my list of most disliked medications, they may overtake beta blockers any day now. One of the problems with these drugs is they cause such severe depression that there have been a number of people who've actually committed suicide. Some people have become very violent while taking them and it's a direct result of the drug. These drugs include Mevacor, Pravadol, Levostatin, I think that's the new name of one of them, and then there's another classification that was before those. Those are the ones that actually get into your liver and interfere with the production of cholesterol. They're really great because they cause liver cancer. But the other classification which is what they call the bile sequestering drugs, things like cholestid and questrin and atromid, those are the ones that keep you from reabsorbing cholesterol out of your gastrointestinal tract. Did you know that cholesterol is such an important substance in your body that you have a whole setup to save it? It's excreted in the bile, your body goes into the gut and reabsorbs back it into the bloodstream because it needs it to make cells, it needs it to make steroid hormones, it needs it to make all your sex hormones, so we conserve cholesterol. And what the bile sequestering drugs do is they interfere with what's called the enterohepatic reabsorption of cholesterol cycle, it interferes, it cuts that off, and so you can't get it back. I was reading in the PDR, I pulled out the 1997 Physicians Desk Reference and I just looked up one of them at random, I looked up Atromid, because I wanted a little more information on this established link with cancer, right? And in the Physicians Desk Reference they use up two columns to tell you that there was this big study with 5,000 patients for five years taking Atromid who had a 44 percent higher mortality than in the untreated group. Wait, the treated people were 44 percent higher than the ones who took nothing, right? And what they died of was malignancies. They were all catching all kinds of cancers, and/or pancreatitis. Now pancreatitis is not a fatal disease unless you're taking one of these drugs. Because what happens with this drug and nobody quite knows the mechanism really horrible gallstones which block the bile duct and then the pancreas just digests itself and it's gone and you can't replace the pancreas, we all know how fatal pancreatic cancer is, right? So the bile sequestering drugs are horrible and the ones that are the cholesterol blocking drugs are even worse because they cause liver cancer. They also as if this mattered can cause constipation, I don't any of us care about that in light of what else they can do, and impotence, and then this vitamin K deficiency is very serious. The majority of our body's supply of vitamin K is made by our gastrointestinal bacteria, that's where we get it , and vitamin K is essential to the clotting mechanism. If you don't have enough vitamin K you bleed to death internally, you bleed out of your capillary ducts. And this causes a really serious vitamin K deficiency and in a lot of elderly people that's what happens they get gastrointestinal bleeding. So I wanted to share with you some of the references on this. And in the New England Journal of Medicine in 1996, they published a study that showed that these cholesterol lowering drugs were no better than a placebo in reducing the risk of heart attack, they weren't doing anything, right? And a study, I love this one, there was a study in the British medical journal in 1996, okay? There actually may be no link between cholesterol and saturated fats and heart disease. Does that blow your mind? How many years have we been told cholesterol, cholesterol, cholesterol, don't eat eggs, don't eat fats, don't, don't, don't, don't, don't? And yet none of the studies have established that link. And I hope that by the time we're done this evening you're going to see how wrong-headed that is, it's exactly backwards, we'll talk about it. There was only one major paper in the last 20 years that has shown any link whatsoever between eating meat and heart disease and it has been discredited, they weren't sure that the way they did the study was all that good. And every other study that they've done to try to duplicate it has not been able to turn up that connection. And in any event quite beyond any of this that it may not even be a connection the Journal of the American Medical Association in 1982 published this article that said lowering fat and cholesterol intake doesn't have any statistical effect on the total plasma concentration of cholesterol. You make far more than you will ever eat because your body needs it so badly. You're not making it casually, folks, so looking at cholesterol as a huge problem is probably very wrong-headed. There's one other thing that I thought was really interesting. There are a lot of public health experts who now believe that universal cholesterol screening is unnecessary. For people over 75 cholesterol levels are not a risk factor for heart disease, not at all. And for men under 35 or women under 45 it doesn't seem to be important. The only time that would be important is if you had a big family history of cardiovascular disease, I mean lots and lots of your relatives died of a heart attack or something, and that you had more than two of the following risk factors: either high blood pressure, smoking, or diabetes. If you're in that classification then the cholesterol level may have some bearing on your likelihood of developing cardiovascular disease. And what did we do? We stopped down at the market and we just had breakfast that's not even a fast and they take your cholesterol and they scare you to death because your total cholesterol level is sky high. I've had people run into my office and tell me "My cholesterol is 346!" I said, "Okay. Now, what was your HDL level?" "I don't know." "Oh, okay. When was this test taken?" "Well, I got a screening done." "When had you eaten breakfast?" "Oh, I just had breakfast and went to the store, it was about an hour and a half." "I see, what did you have for breakfast?" You know, we went through this whole questionä It turns out the test was totally invalid, scared him to death for no reason.
[TOP]
And the two hours after you first eat, your cholesterol level goes really high, it's supposed to. And the other piece about that is have you guys ever had some terrible doctor like me tell you you have to fast for 14 hours in order to take your blood draw? It's because the only valid comparable level of a cholesterol level is after a 14 hour fast. That's how long it takes to equilibrate it so that you can really get the true skinny on how much cholesterol this person makes. And if you don't have an HDL level with it forget it because it still doesn't tell you anything. I have a patient in my practice, she has a cholesterol level of 358 and she has a cardiovascular risk below normal because her HDL's are sky high. They're almost 100. She just has very efficient cholesterol metabolism and she's not at risk for cardiovascular disease. So, please don't be scared by that, alright?
Okay, let's change the tone of this a little bit. Now that we've gone through all of the stuff they want to give us and all of the things that it can do to us, is there a different answer? What's the option? Where do we go from here? If we're not going to go through the medical regime and take all the drugs and do all the surgery what are we going to do? Because if you're worried about it you want to know what you can do for yourself. Well, there's an enormous amount of information about how effective lifestyle change when it comes to cardiovascular disease. Lifestyle change has almost gotten to be like this little catch word. So let's talk a little bit about what we mean when we say lifestyle change. For those of you who were here earlier in the year or did we bring some of those tapes? I have a lecture on cardiovascular disease "Is Your Diet Your Downfall" that goes into this in detail and we have some at the back if you want to hear that in its entirety. The first thing you have to look at is a high fiber diet and when I say high fiber I'm not talking about bran and all this added stuff that people do. I'm talking about fruit and vegetable fiber. Pectin and oats and that kind of stuff, it's soluble fiber. And that soluble fiber has a huge amount of protective value in a way that the drugs do not have. In addition, if you're eating a diet high in fresh fruits and vegetables you're optimizing both your mineral intake and your vitamin intake and I recommend the freshest vegetables that you can get, right? Like the Saturday morning farmer's market here in Pasadena, right, or a good produce store. I get most of mine from Sierra Produce down in Arcadia, it's close to my house. But you're looking for high quality vegetables. Don't skimp on veggies, because if they've been on the shelf for a long time they don't have any food value left. Also a really good high intake of B, I prefer natural B vitamins. Most everything that we have in our diet today are all these enriched flours, enriched with those six synthetic vitamins, B vitamins that they add back after taking out all 38? They're all made from coal tar, they're all petroleum byproducts. Yeah. There is a cadre of people in the natural health field who say that all synthetic B vitamins are poison and that you should never take anything but natural. And in the people that I've been testing I'm finding about 50/50. Some people can take the synthetics and are okay and other people can't touch it because it's really bad for them. That's what the phonocardiogram is good for and we'll talk a little bit more about that in a few minutes. But you want things like wheat germ, remember your mom feeding you wheat germ? My mom did. She always put it in the meat loaf so we couldn't taste it, it's a good way to use it. Um, whole grain, brown rice, that's why everybody says brown rice is good for you? It has B vitamins, right? Molasses, dark blackstrap molasses, that's the B-vitamin fraction of sugar cane. They take all the good stuff out of sugar cane and refine it out and they sell it as molasses and they have what's left and they feed it to us as sugar. Avoid sugar and starches. One of the things we are finding out is that cardiovascular disease is somethingºit's a sub-clinical form of what we would call diabetic dyasthesis. Diabetes has several hallmarks and of the major hallmarks of it is arterial disease. Sky high blood fats and cholesterol because they can't metabolize them properly. Because they can't metabolize sugars properly they don't have the insulin. It's a complicated metabolic pathway that results in diabetic people converting their sugars into fats and those fats then damage the arteries and all this stuff starts to happen, okay? When you eat enough sugar you can induce a diabetic-like condition in yourself because you don't have enough insulin to deal with what you're eating. So tell me something, have you ever read the label on a no-fat pastry? Yeah. How about, what is it, is no-fat ice cream the latest? Loaded with sugar! All we're getting in our culture nowadays is sugar. Would you know that essential fatty acids are critical to the health of the heart. A low-fat diet is the worst thing you can do if you have heart disease. In our latest newsletter I have an article about a man who was set up to have a heart valve transplant and we've reversed it and you know what we gave him? Fat. Salmon oil, blackseed oil, borage oil, all those oils, that's what the heart needs to maintain the health of the arteries and the health of the heart's activity. So I'm asking you to basically to throw out everything you think you know. I'm really challenging that idea. You know, eating a healthy diet in the United States is really a problem, I mean it requires intense effort and attention. My sister who markets for me bless her soul goes to five different markets for me. We go to the health food store, we go to Trader Joe's, oh excuse me, four, we go to the produce market, and then she goes off to Hughes and gets my cat food and paper products, right? I don't think there's anything to eat at the supermarket. At least there's nothing healthy anymore. Processed food will be the death of us, I'm thoroughly convinced by that. So we want a high intake of our B vitamins, we want a high intake of the antioxidants including A, E and C. Well where do you get these? You get them in whole unprocessed foods. Everything we're talking about here comes from an unprocessed food source, not from something that's on the shelf and won't spoil because they've processed it so far. Especially magnesium. Do you know that magnesium is the most effective antiarrhythmic drug there is? It's more effective than digitalis or digoxin. You can bring an arrhythmia under control faster with magnesium than you can with the drugs? But we don't here about doctors in the hospital giving anybody a magnesium infusion, do we? And it has absolutely no side effects. If there's anybody in the audience who suffers from mitral valve prolapse, they have a magnesium deficiency. That's what it is. And all those symptoms about anxiety, and all that stuff that goes with it, magnesium deficiency. Magnesium is estimated to be the most commonly deficient mineral in the United States. And the reason? It's dark green leafy vegetables. How many people these days eat dark green leafys? Right, kale, me, too, I love them, kale and brussel sprouts, you know, all those good things. It's just not that common in the American diet anymore. This is the same problem that we're having with our essential fatty acids, especially the omega-3 fatty acids. Omega-3's are our fish oils, right, we think of them as fish oils. Well, the sources of omega-3 fatty acids include: dark green leafy vegetables, chia seeds, pumpkin seeds, flax seeds, herring, cod, salmon, and sardines. How many of those have you had recently? Show of hands? Yeah, me, too, good, good, good. People have been listening, I'm glad to see that. And if you're going to go the vegetable route, the vegetarian route, if you're not going to eat the fish oils, you need anywhere from 100 to 1,000 times as much because the conversion is not very efficient. Um, especially if you don't have the proper B vitamins which we already know are so deficient, okay? CoQ10 is one of those magic enzymes which is touted as a help with people with heart disease. Again with my phonocardiogram I'm finding about a third of the people really need it, the rest you find with enough vitamin E and CoQ10 is so expensive we stick with the vitamin E. Um, the most important thing you can do for yourself in terms of vascular disease of any kind, is to avoid hydrogenated fats and oils. These are margarines, these are Crisco, these are soft batch cookies and you read and it says hydrogenated vegetable oils. Read labels. Please read labels. Everything has hydrogenated vegetable oils in it. And the trans fatty acids that are produced when they hydrogenated vegetable oils are believed to be the single most serious cause of cardiovascular disease because the body cannot metabolize them. There's absolutely no way they can break them down. And they do serious damage to the heart. I have lost my copy of this slide. Here it is, I put it back before I was ready, excuse me. Weight loss to control blood pressure. Okay? It's been proven that if you lose weight your blood pressure will go down, there's no question about it. But if you're like me and you're built a little bit large and you walk into a doctor's office and somebody pulls out a standard blood pressure cuff and tries to take your blood pressure, stop them. Make them go get the large cuff. I am just shocked by how many people have inaccurate blood pressure readings because nowadays we have nurses and physicians' assistants doing all the exam and intake and they don't know that the blood pressure cuff has to go two thirds around the upper arm or the blood pressure reading is invalid. I just got over pneumonia, right? I walked into the doctor's office, they take my blood pressure. They put a standard blood pressure cuff on me. This lady is like, you've got hypertension. I said, wait, you're wrong, I have extremely low blood pressure, would you please go and get the other cuff? And she did and sure enough, my blood pressure was 112/60, they didn't quite know I was walking around, and neither did I, to tell you the truth. But watch that, okay, don't get a misdiagnosis because somebody's not used the equipment properly. Make sure that they are really taking the right reading. That's very very important. It takes them a few extra seconds but what does that matter? It's your blood pressure. Now chelation therapy has been shown to be enormously effective, especially in coronary artery disease. Um, this is not a lecture about chelation therapy, but I have in my office a reference of doctors all over the United States who do chelation therapy because chelation therapy will clean out the arteries faster than anything. It's been proven time after time after time and when I have someone in my office who has really bad coronary artery disease, I recommend they do that first. Go get chelation, and then make the lifestyle changes because the chelation will buy you time. It will clean those arteries and then if you make the changes they won't clog up again. You can reverse it if you take the right actions. Unfortunately, I'm going to make an attitude statement here, the only people that the medical profession hate worse than the chiropractors, are the medical doctors who are doing chelation. I have a book in my office written by one of them called Medical Racketeering, gosh, I thought we had troubles until I read that book. And you're probably all aware at this point that the Mediterranean diet lowers the risk of heart trouble. This was published in the American Journal of Clinical Nutrition 1996, there's been a lot of emphasis placed on that. Unfortnately they're focusing on the wrong part of it, they're focusing on the pasta. Mediterranean diets are not heavy on pasta. Pizza is an American invention, none of my relatives in Italy knew anything about it. The Mediterranean diet is lots and lots of fresh vegetables, lots of olive oil, lots of fish, so it's really a very healthy healthy diet that contains a lot of the things that we've been talking about, vegetables, vegetables, vegetables. I'm going to keep saying it, not hitting her favorite button here, which is great. I love the reaction, I understand that, and yet they're the highest nutrient source we can eat, veggies are really good for us.
[TOP]
Now in the New England Journal of Medicine in 1993 they actually published two studies that showed two studies that showed that just vitamin E by itself decreases the risk of heart disease by either 26 or 46 percent depending on which study you look at and that's really pretty amazing. Do you know that there are no good sources of vitamin E in the American diet? Do you know where our sources of vitamin E are? Wheat germ, and egg yolks. How many people eat either of those things anymore? It's like, we've been warned off of the very foods that could be saving our lives. It's just that simple. And there are specific portions of the B vitamin complex that are very heart active, they have specific effects on the heart cycle.
A book was published in England by Arrow Publishing called The Heart Revolution by Dr. Paul Sherwood. And to read his quote in its entirety, he said, "Many coronary attacks are the result of an old injury which has jolted or twisted the upper part of the back, giving rise to serious repercussions throughout the whole body. The muscles of the back by contracting actually pump blood back into the heart and after injury they remain in a continuous state of spasm making them unable to pump efficiently. Over the years the damage accumulates and begins to effect the heart. " So musculoskeletal injury causes heart disease. We've known this in the United States in the chiropractic profession for a long time, as early as 1920 there was a study a pathology study done at one of the big medical schools, I think it was Columbia medical school, don't hold me to that, I think it was Columbia. They did an autopsy thing and they were able to trace organ disease back to specific levels of the spine and show that there was all this fibrosis and scarring and just the whole spinal area was trashed and they did that with like 250 or 300 cadavers. So there's a really strong connection there but we never hear about it in the United States of course. We never think of it in those terms. And then they did another study in Finland and it was published again in Britain in the medical journal there in 1994 and they documented a link between back pain and the risk of fatal heart disease and the people most at risk are men in the 30-49 year old category and of course that makes sense because guys work really hard. You know, I have so many young men who come in, they think they're invincible, they just try to pick up the refrigerator by themselves, and years later they end up with heart trouble.
So I want to talk just a little bit now about the phonocardiogram. That's not exactly what it looks like, this is what it looks like, but that was the closest I could come in my clip art, okay? This machine is really quite amazing. It was developed by Dr. Royal Lee who was not an M.D., he was a dentist and he was an inventor. It's amazing to me how many holistic kinds of practices have been invented and promoted by dentists. In 1937 he designed this machine, he called it the endocardiograph. And basically what it does is it charts the heart cycle. Now, you know, I don't know, maybe you don't know, but you can listen to the heart, but it's really hard to distinguish the heart cycle. It's hard to tell what's the first heart sound and what's the second, it kind of runs together. It's hard to make the fine differentiations, anybody can hear aortic stenosis, it sounds like a fssshh sphhhh, you can't miss it, but a lot of these other things are more subtle than that. So what this machine provides us with is an actual picture of how your heart is working. And then you can sit down and you can analyze different features on the strip and you can then know what exactly is going on with this particular person's heart. It's a momentary snapshot of the heart. Now, if you have an electrocardiogram and your ECG was perfect and there was nothing wrong and there was no heart damage, that's great. But that's all the electrocardiogram can tell us, it's history, did I ever have a heart attack, that's what it will tell you. Do I have heart block, do I have conduction problems, it doesn't tell you how the heart is working in the moment. And when you stop to think about it, the one organ in your body that never rests is your heart. It beats every moment of your life and the minute it stops beating, I'm sorry, but we've lost you. And so it needs the best possible nutrition, this is where the cardiovascular system comes into play because the blood supply to the heart is critical. It has huge oxygen demands. So you can immediately see changes in the heart cycle simply by putting the nutrients under the tongue in contact with the capillary bed, you know that purple under your tongue, that's a capillary bed, it goes straight from there into the brainstem and affects the heart cycle, just that fast, 30 seconds, and you can see the changes. I tell you, I'm having the most fun with this. I've been doing this kind of healthcare now for what is it, 12 years? Something like that. And I've been blood work and giving people nutritional programs based on blood work based on at least 7 or 8 of those years. With this, I can take what their blood work says, run one of these, find out what else is going on, test everything, and we might start out with a big list and we come down to the list of just what that person needs. And we can immediately tell do they need synthetic B vitamins, do they need natural ones? I mean, you can just lay it all out. It is so fun. Having great fun with it, and I've had some remarkable turnarounds in people thatºI had a man with what is called malignant hypertension, malignant hypertension is a systolic pressure greater than 200 and a diastolic pressure greater than 160 and he was well over that. And it means that you're probably not going to live two years. Well, his blood pressure is now totally normal. He gave us this little story for our journal. He wouldn't take the medications, they weren't lowering his blood pressure, and he felt terrible when he took them. We put him on a nutrient schedule and he's back to 100 percent. So it's been fun, even for me when I know what's possible I'm still surprised by it.
Now at this point we may digress into more than you ever wanted to know about the heart. I want you to at least see what I'm looking at when I take one of these readings. This is an example of the heart rhythm and the heart cycle, I don't seem to have my pointer but that's okay. If you'll look at the section, A, B, C, D and E, do you see that going across the bottom, those sections there are the activity of the valves. In the A section the heart valves are open and the mitral or tricuspid valves are just preparing to close. So there's this little preparatory noise that you see as that initial spike on the dark black graph. And then in the B part of the cycle the S1 has closed and, the mitral and tricuspid have closed and the big valves, the aortic and pulmonic are wide open. And then we go through the resting part of it, I means, backwards, I do this all the time, we're going through that contraction when they're squeezing all the blood out of the ventricles which are the aortic and pulmonic, right? And then as the heart relaxes in our D section the blood comes back and the valves slam shut and that's the last part of the sound, the shutting of the aortic and the pulmonic. So that's what you're looking at when you look at a graph on somebody. Let's go to the next slide. What we do is we put our little stethoscope on the areas where the valve sounds are the loudest, that's what that graph is, that shows you the relative position of the heart and where to put your stethoscope so you can get the best heart valve sounds. When you do that, you come out with something that looks like this. This is a totally normal graph of all four of the heart valves, the aortic, the mitral, the pulmonic, and the triscupid. If you look at that graph for just a moment, you'll notice, S1 is tall and straight, it's kind of close together, and the second heart sound is smaller, it's supposed to be a third of the size of S1, and also, nice and tight. Let's go to our next slide. I don't expect you to be able to read phonocardiograms when we're all done with this so I'm not going into detail with it the way I do with the doctors that I teach. These are some graphs of people who had heart troubles. That was good. The first one, if you'll notice this graph, this person does not have a tall S1. You notice how we had seen, look down at the aftergraph, you see tall and spiky? The top one looks kind of cutoff, like it's not quite high enough and it's not working really good and you may also notice that it's broadened, it's elongated, this is a graph of somebody who needs Cataplex B, which is the water soluble portion of the B complex. You put that under their tongue and instantly their heart graph normalizes, you see the change there? And these people have things like arrhythmia or fibrillation, a heart block which is a delay in the heart cycle or sometimes they'll skip beats. And you can give them Cataplex B and it turns around right away. The one below which is Cataplex G is the alcohol soluble portion of the vitamin B complex. It has an entirely different effect on the heart. These are the people who don't have a long enough resting cycle. What's supposed to happen is you're going to go, "Lub dub, pauseº(the heart's resting), Lub dub, pauseº" That's why they talk about athletes with that beat of 50 to 60 beats a minute that this person's in good condition? Because their heart's resting a lot in between it's getting a good rest and lots of oxygenation. People who have problems in the heart, things like angina and heart failure will often have what we call almost a tic tock rhythm, it's lub dub, lub dub, lub dub, there's no rest in between their heart cycle. And the result of that is they're not getting good filling in the coronary arteries, the heart's not getting a good chance to oxygenate, it's just working too hard. And the alcohol soluble portion of the vitamin B complex will actually increase, we call that the diastolic index. It will increase the resting time in the heart, it's amazing to watch it happen.
[TOP]
There is a condition where the second sound is higher than the first. This is a person who has something that we call functional pulmonary hypertension. This has been in the news a lot, this is Fen Phen, Fen Phen does this. And it's actually an adrenal problem, the adrenals are not working well, and that's the cause of the functional pulmonary hypertension. By giving the appropriate adrenal support, that's what Drenamin is, you could actually turn that around. Now you're not going to see instant results with this, it takes longer, because rebuilding the adrenals is a longer term process, but you will see the heart start to switch over just as you put it under your tongue. Yesterday I did a phono on somebody and I actually brought hers back to normal with the right nutrients. She had terribly high second heart sounds they were probably three times higher than S1 and with the right nutrients they were totally normal. It was really exciting to see that. The lower one is a fairly serious condition where you have a person who's heart is not working well at all, this is a heart that's just not getting enough oxygen and so the heart rhythm is disorganized. This Cataplex E2 which is a special fraction of vitamin E and actually from green peas? Takes likes a cross between green peas and hay. I take it when the smog is really bad. Chewing it up is the most effective way to take it and honest it tastes like stale green peas and hay. That's all I can tell you. But notice what it does for the heart. The contractions are coming back. This is a person who is instantly feeling better. And let's look at the next one, because the first one on here is very important to me. This first graph up at the top, this is a person, you notice there's almost no second heart sound there? They're not using their calcium well. You know, they could be taking lots of calcium, but it's not getting to their heart. There's a whole system whereby their heart impulse is dependent up on the flow of calcium ions in and out of the calcium channels. That's the mechanism of action remember those calcium channel blockers? That's what they act on. Well this poor person isn't able to use their calcium appropriately so they have a weak S2, that means their primary heart valves are not closing effectively. You're getting poor blood circulation and you're getting a lot of regurgitation back into the heart, okay? So we give them Cataplex F. Do you know what Cataplex F is? Essential fatty acids. Does that sound familiar? Look what happens to the heart, almost immediately the heart starts to strengthen. You see a good S1 and the S2 is reasserting itself. I mean the results are dramatic, it's really really something.
We have other examples of other less common conditions. So in summary what I'd like to tell you is that there are a lot of very kinds of common sense, nutritionally based safe ways to be healthy. You don't have to go for the most invasive and in the case of cardiac medications the most dangerous options. This is not to say that I have never referred anybody out to a cardiologist for care because I have. There are people who are not candidates for this kind of healthcare because they won't take care of themselves. They won't take the extra effort to eat the right thing or to take their supplements or they'll tell you that's too many pills. But if that's the way the person's going to be, then we don't need to ºI'm not going to try to help them because they're setting themselves up for failure. But for people who want something better with what I consider to be a very much better outlook this is the option that is available.
Does this apply to you? If so, see our information on Consultations.
[TOP]
© 2011 Richards Family Health Center. This site or any part may not be reproduced without the written consent of Richards Family Health Center. N Rowan Richards, DC, DABCI, FIACA at 242 South Glendora CA 91741. 626 963 1678. email:richardsfhc@richardsfamilyhealth.com. This site is Not intended to dispense health advice or serve as a substitute for actual patient contact with a qualified healthcare provider. Our sole purpose is one of education. It is our expectation that our site can educate our visitors about the efficacy of some healthcare treatments that exist as an alternative to conventional medical wisdom.
PRIVACY POLICY: Richards Family Health Center takes your privacy very seriously. Be assured that we do not sell or rent your contact information to anyone.